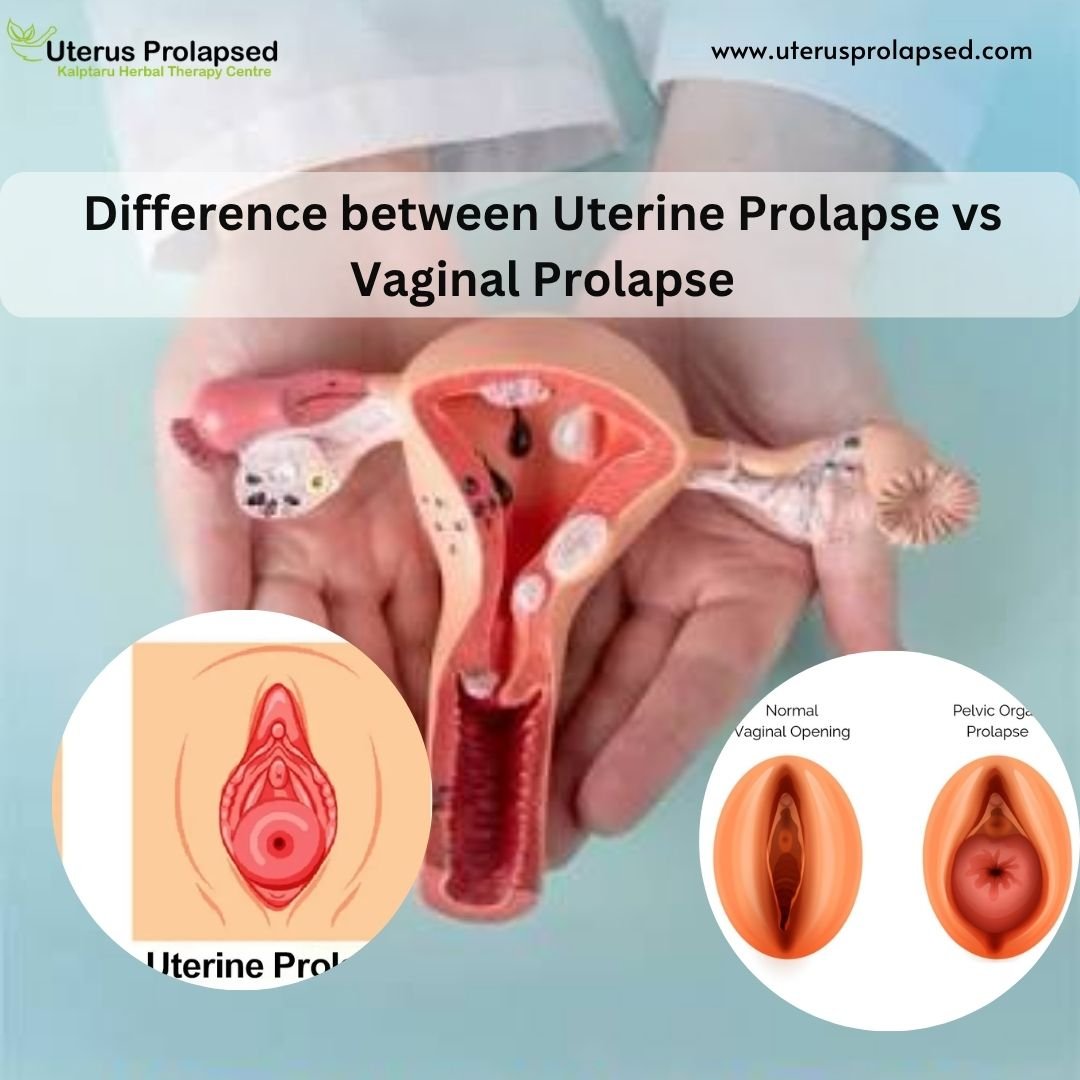
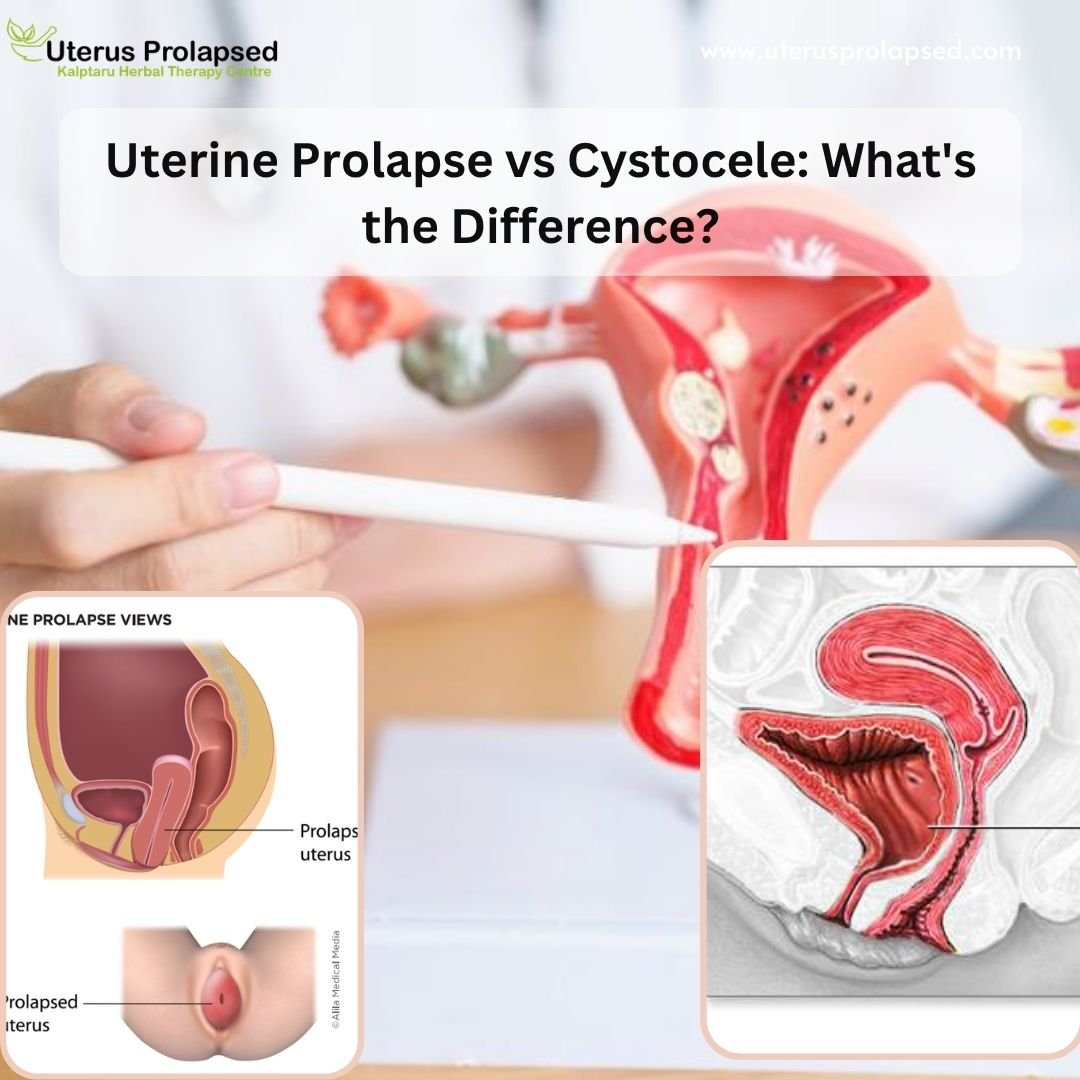
Uterine Prolapse is the descending displacement of any pelvic organ from its usual position. It generally includes the womb and along with-it bladder or rectum may also be tangled. Complete pelvic organ prolapse is recognized as Procidentia.
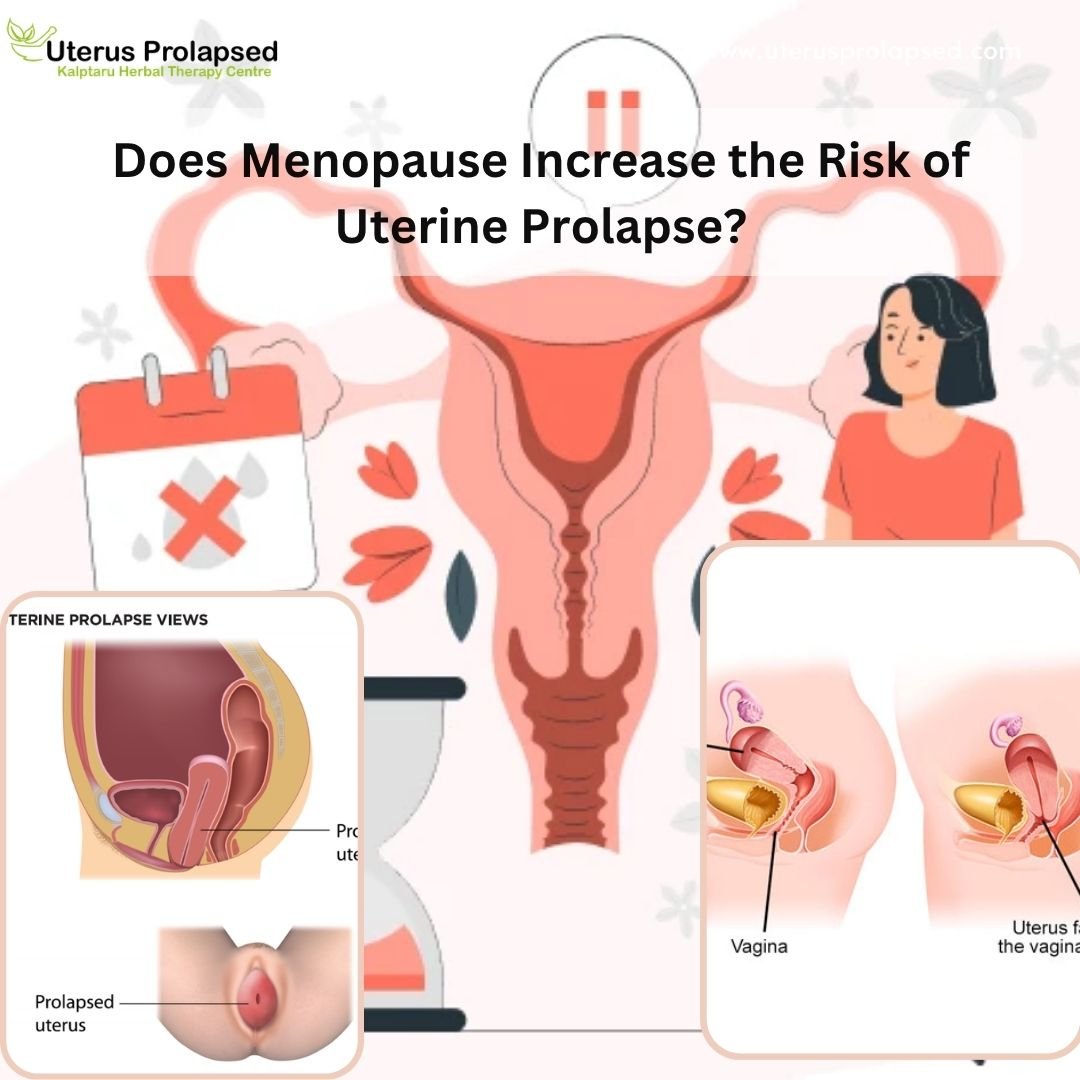
Uterine Prolapse is most frequently accredited to childbirth injury or it may be due to the inherent dimness of suspensory tendons. Prolapse manifests most usually after menopause when the production of ovarian hormones slowly stops and genital provision weakens.
A uterine prolapse happens in numerous stages:
- First-Degree Uterine Prolapse: In this circumstance, the cervix drops into the vagina
- Second-Degree Uterine Prolapse: In this case, the uterine cervix is just at the opening of the vagina
- Third-Degree Uterine Prolapse: In this circumstance the cervix outside the vagina
- Fourth Degree Uterine Prolapse: also named as procidentia, here the whole womb is outside the vagina
Treatment/Management of Prolapsed Uterus
Treatment of uterine prolapse is mainly dependent on the extent to which a patient is undergoing symptoms. Treatments contain surgical and non-surgical choices, the choice of which will depend on overall health, the sternness of the condition, and plans for future gravidity.
Proper analysis and management of uterine prolapse can majorly affect a patient’s quality of life and can have long-term physical and mental well-being effects.
To stop prolapse, you could accept the following measures:
- Treating and preventing constipation
- Performing Kegel workouts frequently
- Avoid lifting heavy weights
- Controlling body heaviness
- Vaginal pessaries: Objects frequently made of silicone that are interleaved into the vagina to offer provision for the prolapsed pelvic organs.